Pediatricians Adapt to Changing Attitudes Toward Vaccines
In a new era of parental vaccine hesitancy, how can physicians rebuild trust?
- 12 minute read
- Perspective
Illustration: Blake Cale

Illustration: Blake Cale
Let me give you two pediatric moments from 2025.
Moment number one: a spring afternoon. I was sitting in the teaching area of the pediatric clinic at Bellevue Hospital in New York City with a group of faculty colleagues, all of us waiting for the residents to come and tell us about the children they were seeing. A news flash came in on someone’s phone: A child in Texas had just died of measles.
Every pediatrician in the room felt it as a blow: The thing that must not happen has just happened. During my pediatric training at Boston Children’s Hospital in the 1980s, I never saw a case of measles. I saw children die from many different diseases but never from measles. Measles was gone, not eliminated from the face of the Earth, like smallpox, but no longer endemic in the United States. It did not threaten our patients in Boston. Our patients were vaccinated. But in the spring of 2025, a measles epidemic was raging in Texas. And yes, children died.
Moment number two: the opening plenary session of the National Conference of the American Academy of Pediatrics (AAP) in September. We had just sat down after listening to the Denver Children’s Chorus sing the National Anthem. Susan Kressly, a pediatrician and the current president of the AAP, asked us all to stand up again and scream. Some 5,000 pediatricians, in a giant conference center auditorium, let loose and howled. We all understood why we were screaming — in grief, in pain, in outrage, in anxiety. “It’s not been an easy year for our members,” Kressly said.
But in addition to that cathartic stand-and-scream, the national pediatric meeting was notable for moments when we applauded like we would never stop. Here are some of the big applause lines for an audience of pediatricians in the fall of 2025: a video of the next AAP president, Andrew Racine, a pediatrician at Montefiore Einstein in New York, saying, “Vaccines don’t save lives, vaccinations save lives.” We cheered so loudly that we drowned out the next lines of the video. And you should have seen the moment when Kressly thanked the AAP infectious diseases committee and called them “guardians of truth.” It stopped the show.
I started my pediatric residency in July 1986 and almost immediately began to identify as a pediatrician, well before I could claim any real skill or experience. In pediatrics, I had found my people. I wanted to be part of that particular us — and I still do.
I worked for years at a neighborhood health center in Boston, with a population made up of new arrivals (Vietnamese refugees, Haitian immigrants) and longtime Bostonians. I worked in the refugee clinic at Boston City Hospital. Now I work at Bellevue, the oldest public hospital in the United States. The people who came to those places wanted vaccines. In many cases, they were downright eager to have their children vaccinated. They were grandmothers who remembered bad diseases in the old country, wherever that was, or parents who remembered systems in which vaccines cost money. They were the descendants of longtime neighborhood activists who had fought to bring the health center to the community so that kids could get their shots close to home. They were refugees eager to send their children to school in their new city who looked at the completed school health forms as tickets of opportunity.
I knew there were people out there who didn’t trust vaccines, and to be honest, I was grateful not to be taking care of them. I remember, more than a decade ago, speaking with a woman from Marin County, California, who had given birth to very premature twins. After a long and difficult few months in the newborn intensive care unit, she had finally brought home her precious, delicate babies, but it was flu season, and she worried obsessively that they would catch a respiratory virus, that they would be rehospitalized, that they might even die — all perfectly reasonable worries for a parent in her situation. She, of course, had gotten her flu shot as soon as it was available, as had every other member of her family, but the twins were under six months old, too young to get the vaccine, and she was aware every day that she lived in an area where many people refused vaccines. How could she tell which neighbor might casually bring disease into her house, which passing stranger who admired her babies in the park might be breathing death?
Vaccines don’t save lives, vaccinations save lives.
I remember this conversation because I agreed with her, and because I felt a mix of disapproval and scorn: Rich Californians, what can you expect? That was, to be honest, the way I had always thought of what we now call either “anti-vaxxers” or even “vaccine-hesitant” parents: They were entitled and overprivileged people who felt that other people’s children should be vaccinated, which would then protect their own precious and entitled offspring. They thought they ought to be, if you will pardon the expression, immune.
In contrast, the patients I took care of had parents who really got it. Some came from parts of the world where they had seen the diseases we were vaccinating against — measles, polio, neonatal tetanus — which was certainly more than I had ever done. But whether they were immigrants or born in the United States, the parents I worked with only very rarely expressed any anxiety about immunizations. When stories about vaccine hesitancy came up, my colleagues and I would look at one another and shake our heads, feeling fortunate that we worked with sensible parents, parents who wanted to protect their children and their communities, parents who trusted us.
But now, the stories I hear from old friends and colleagues in pediatrics across the country make clear that something has changed. Terri McFadden, a professor of pediatrics at Emory School of Medicine, started practicing in 1991 and has worked with the same population ever since — “an urban underserved population, mostly people of color.” Like me, she remembers a time when it was very infrequent to have a parent who decided not to vaccinate, she says, “and even then, you could have a conversation. Now, I find, there is a group that is just not going to vaccinate. … They’re just angry.”
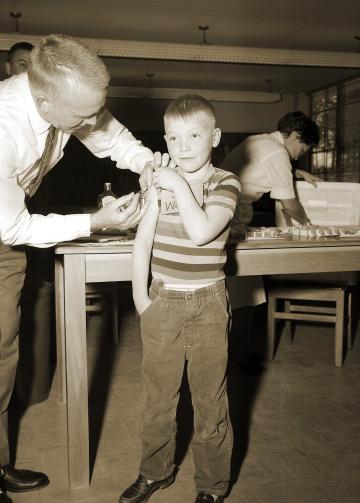
Photo: Smith Collection/GADO/Getty Images
Amy Shriver, a general pediatrician in Des Moines, Iowa, has been in practice for 17 years, working with an urban population, mostly children on Medicaid. Recently she saw a family two days after their baby had been discharged from the newborn nursery, and she read in the baby’s chart that the parents had refused to have the newborn screen done. This blood test checks for a large number of genetic problems, many of which can be treated much more effectively if they’re found early. There’s no shot involved, no injection of any kind, just a blood test to look for danger. She asked why they had refused the screen, and “they said they just didn’t trust the system, they didn’t trust any of the testing, and no matter what I said I couldn’t explain why it was so important.”
We are seeing more of those angry families, who come into the exam room knowing that vaccines are dangerous, that greedy pediatricians are in league with maleficent pharmaceutical companies. “I’ve had conversations about how vaccines are coming up where people will appear to be vaccine hesitant with good questions and then the questions devolve into an anti-vaccine attack on pediatricians — in my exam room!” Shriver says. “One new family came to me with a 2-week-old baby and the dad wanted to know why there is no mechanism for people to sue the vaccine companies and why we give so many vaccines at the same time.” Conversations like this, she says, “leave me feeling tired, defeated, and mistrusted.”
So what happens with a family like that? “I almost didn’t want to see them again. I said, ‘I’m happy to provide you with evidence-based information, and please ask me more questions,’ but in my heart, I didn’t want more questions.” She pauses, then adds, “They didn’t vaccinate at the two-month visit, but they saw me again.” And she adds that she feels strongly that all children deserve high-quality care, whether their parents decide to vaccinate or not, and therefore “I will continue to see all children and work on relationships, hoping that things might change.”
McFadden points out that families are bombarded by misinformation, and that our medical system does not make it easy to maintain the relationships between patients and doctors that build trust over time. “I feel like it’s harder and harder to have the continuity with families that builds that trust,” she says. And the lack of trust extends beyond vaccines, to the recommendations that we make about how to protect children from other dangers, about safe sleep, about limiting screen time. “Families are feeling that we don’t understand their lived experience,” she says, “that we don’t understand what it’s like to be a parent in 2025.”
Parents are also being targeted by purveyors of disinformation, with scare tactics often aimed specifically at vulnerable communities. At Bellevue, we have lots of parents who refuse the COVID vaccine and the flu vaccine. We don’t often see the angry parents, but more and more, we see parents who say they don’t want vaccines. We don’t turn away unvaccinated children (we don’t turn anyone away), but we do point out that they will need to be vaccinated for Head Start and for school. We encourage the residents to have these conversations, over and over again, and we congratulate them when a hesitant family agrees to vaccinate. It used to be something that came up once in a while in the clinic, an interesting “teaching case.” Now it’s every day. It’s something of a burden — these conversations do take time — but it’s a skill that the residents need to practice.
For my part, I find that now, I talk about vaccination in every class I teach. I have come to feel that it is something that everyone needs to understand, this incredibly clever human trick, in which people learned to turn on an immune system so complicated that when you diagram it, it quickly comes to look like a parody. Vaccination is named for the cowpox virus, vaccinia, the mild virus which reliably sets off the smallpox immune response, triggering the development of a false memory. It’s a name — and a process — that celebrates human cleverness.
Paula Prezioso, a pediatrician who works in what she describes as a “diverse private practice” in New York City, with offices in Manhattan, Brooklyn, and Queens, has been in practice since 1991. She points out that anxieties about vaccines are nothing new. When she started in practice, she says, people were worried about the pertussis vaccine, which protects against whooping cough; instead of the DPT, they wanted a DT. Then, some years later, there was a furor over the measles vaccine. And then there was the COVID vaccine. “Every few years we have this conversation about vaccines,” she says.
Prezioso tries to emphasize that the conversation about vaccines is important but also part of the bigger conversation about a baby’s health. “We have the conversation about feeding and growing well and eating well and sleeping well and making sure they’re protected against ever-present diseases,” she says. She offers parents sources for reliable information, and she tells them to go home and talk about it and come back with questions. And very few parents, after having the full discussion, refuse to vaccinate.
If they do, I ask, if they do come back and they still refuse? “I tell them we have children in the practice who are immune compromised, parents in the practice who are immune compromised, children who are cancer patients, liver transplant patients,” Prezioso says. “I tell them, ‘I can’t have you bring measles into my waiting room.’ And most of them say, ‘I didn’t think of that.’” So if it’s still no, the family is told that this is not the place for them. “And 99 percent of the time, they say, ‘Let us think about it,’ and they come back and do the vaccines.”
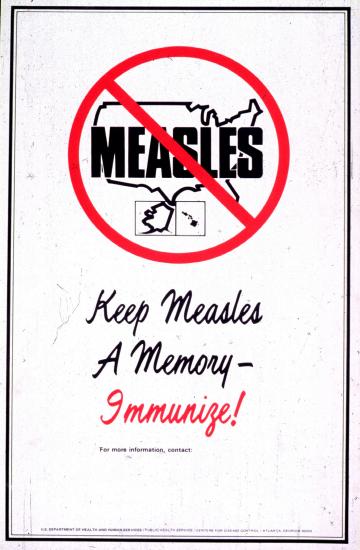
Image: Smith Collection/GADO/Getty Images
But most clinics and health centers can’t turn patients away. Marny Dunlap has been practicing pediatric primary care for 25 years in a community clinic in Oklahoma City that serves Latino families, 90 percent of whom are on Medicaid. “In our community over time, more and more of our private practices have been not accepting unvaccinated children, and so that means we are starting to see more of those families,” she says. People tell her that her clinic is on a list they got from Facebook of practices that will see children who have not had all their shots: “I’ve definitely had moms say, ‘I still appreciate your taking care of my children even though I choose not to vaccinate them.’”
So how does she frame the discussion with those parents? “I still say, ‘As a pediatrician, I highly recommend vaccines. I think they’re safe and effective, and I understand you’re not interested, but I’m going to recommend them every time you come.’” She asks them to sign a waiver, documenting that the subject has been discussed. The clinic has signs up asking if anyone has a rash or fever.
Her own standards have changed, she says, and she has become much more willing to give vaccines on altered schedules: “Giving any vaccine, even if not all on the recommended schedule, if I can get some and then all over time, I now consider this a win, where five years ago I wouldn’t.” Like Shriver, she has learned to sort the patients, distinguishing between those who are vaccine hesitant, with genuine questions, and those she calls “vigilant,” determined to allow no vaccines. “With the truly vigilant ones, I make the recommendation at every visit, but I haven’t had a single one that I’ve ever changed their mind.”
Marsha Spitzer, a general pediatrician at a community clinic in San Diego, was quizzed by one family about why a polio vaccine would be necessary for a 2-month-old. They wanted to know all about the transmission and symptoms of polio, she says, “and I realized I don’t know that, because in my lifetime, I’ve never had to worry about diagnosing polio, and I had to explain, these diseases were eliminated.”
I can’t have you bring measles into my waiting room.
None of the doctors I’m quoting are giving up. All of them feel that the relationships they’ve built with families over time can help protect children. Shriver says that a family she knew well just had a new baby and refused the hepatitis B vaccine. She had cared for all three of their previous children, and they had never before seemed troubled by vaccines. “The mother said, ‘I was just really scared by what I was reading online — I wanted to talk to you,’” Shriver recalls. The mother ended up deciding to give the baby the vaccine.
Spitzer says, “What I’ve always done that feels comfortable to me is, I say, ‘I want what’s best for your child, and you as the parents also want what’s best. It sounds like we might not agree, but let’s continue talking. I am here to support you and your child.’” That takes the antagonism down a notch, she says, and though some of her patients are absolutely adamant, an equal number say they’ll think about it, or they’ll start next visit.
So where does that leave us?
At the national conference, I went to a session on talking with vaccine-hesitant parents. Perhaps not surprisingly under the circumstances, the room was overcrowded and many of us had to sit in an overflow room. Sean O’Leary, a pediatrician and chair of the AAP’s Committee on Infectious Diseases, exhorted us not to normalize vaccine hesitancy. The vast majority of parents in this country are still immunizing their children, he said. Although he encourages clinicians to address parents’ concerns about vaccines, he advised pediatricians to start conversations in a presumptive fashion when talking with parents — that is, to say, “Suzy is due for three vaccines today,” rather than, for example, “How are you feeling about vaccinations today?” We also heard the roar of applause when O’Leary said, “Vaccines are not an appropriate place for shared decision-making — they are the standard of care.” Another big-time applause line, at least for this particular audience.
Meanwhile, pediatricians and practices are coping with a new reality. I do have some colleagues and friends who have stopped practicing primary care pediatrics in part because those conversations were making them crazy. Dunlap says that during the measles epidemic, her clinic was screening all patients for fever and rash by phone before deciding whether to schedule a telehealth or in-person visit. Spitzer is telling parents who don’t immunize their children that if they go to an emergency room or an urgent care center, they should let the doctors and nurses know this, “so they will know to think about some of the things we don’t usually see in pediatrics.”
Closer to home, Prezioso, the doctor in private practice in New York City, is also the pediatrician taking care of the small child whose welfare I take most personally — my 2-and-a-half-year-old grandson, Felix. And although Felix is, of course, now vaccinated against measles, I have to tell you that I found it retrospectively comforting to know that when he was under a year — too young for the measles vaccine but also at the age where measles is most likely to be really dangerous — his pediatrician’s office was trying to keep children who were more likely to have measles out of the waiting room. They were trying to keep my grandson safe until he was old enough to be immunized — and very unfortunately, that meant protecting him from other children who were, themselves, not protected.

Perri Klass, MD ’86, is Professor of Journalism and Pediatrics at New York University, where she directs the medical humanities minor. Her most recent book, The Best Medicine: How Science and Public Health Gave Children a Future, is an account of how changes in infant and child mortality have affected society, pediatrics, and parenting.