On Speaking Terms
In the clinic, making oneself understood is one thing. Knowing what the patient is saying—really saying—is another
- Feature

Douglas Kelling ’72 was born and raised in rural Missouri, which he pronounces “Missoura.” Calling it either “Missouri” or “Missoura” is a regional quirk, determined, some say, by whether you’re from the eastern or western part of that state. As regionalisms go, it’s trivial when compared with those Kelling, now an internist at the Carolinas Medical Center–Northeast in Concord, North Carolina, faced when he entered Harvard College in the mid 1960s. There he learned that water fountains were “bubblers” and that a milkshake lacked ice cream, unless it was a “frappe.” During his internship at Duke University Hospital, Kelling discovered that, despite his Ivy League credentials, communicating was becoming more, not less, complex. One night in the emergency department a man arrived in distress. In describing his symptoms to Kelling, he added, “I’ve lost my nature.”
Kelling didn’t know what to say. In fact, he didn’t know what to ask. “I thought he was heading toward some kind of psychological problem,” he says. Kelling excused himself and asked a resident if he’d ever encountered that phrase before. He then learned that “losing one’s nature” was a regionalism for erectile dysfunction.
Words. Communication’s greatest offenders.
Doctors spend years learning how to effectively diagnose patients, a process that is equal parts art and science. In addition to reading lab reports and feeling for lumps, they also need to pick up nuances of mood, gesture, and expression. Call it the art of noticing. Medical schools understand this and often use creative ways to instill this skill in students, such as with visits to art museums where students are taught to defamiliarize themselves with what they perceive in order to see in new ways.
But what about language? Medical schools teach the arcane vocabulary of biomedicine, and yet physicians often care for patients who speak in other idioms. Simply put, different people have different words for the same things. This fact profoundly affects the patient-doctor relationship.
What’s That Again?
“Losing one’s nature” isn’t the only new phrase Kelling has picked up. There is “smiling mighty Jesus” for spinal meningitis, or “old timer’s disease” for Alzheimer’s. “Fireballs” are uterine fibroids while “strutted feet” are swollen ones. “Locked bowels” call attention to constipation. “Tentacles” are, of course, testicles. There are more; many, many more.
“It’s clear from our research,” says Joan Hall, the chief editor of the Dictionary of American Regional English, or DARE, “that people still use hundreds of regional terms for ailments and diseases. Doctors are often totally unfamiliar with those terms. This unfamiliarity can make patient-doctor communication extremely difficult.”
DAREbegan in 1965 when the American Dialect Society recruited a group of 80 field workers, dispersed them within selected communities, and had them collect regional terms, cataloging, for example, that a pan is a skillet is a spider. This historical dictionary project, always expanding, always changing, continues to this day. Its editors seek the earliest written examples for a phrase and trace the evolution of its usage.
Hall herself is a living, breathing wellspring of lexical exoticisms. She effortlessly references “pipjenny” (pimple) and “salt rheum” (eczema) and can nod sympathetically to anyone who is “rifting” (belching) or has “jags in their leaders” (sharp pains in their tendons and ligaments).
Lest you think potential misunderstandings are trivial, consider this. In 1995, one of Hall’s DARE colleagues was contacted by a psychiatrist in Chicago who treated patients suffering from aphasia, a neurological disorder in which one loses the ability to express, or comprehend, speech. The doctor had questions about a handful of strange terms.
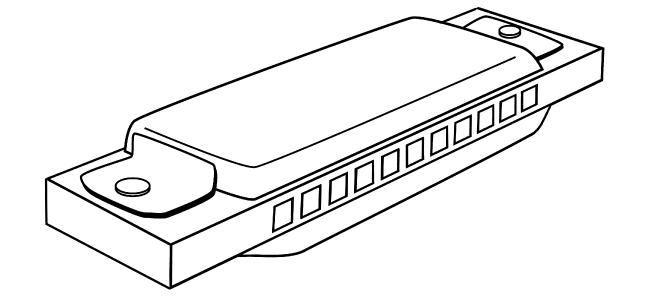
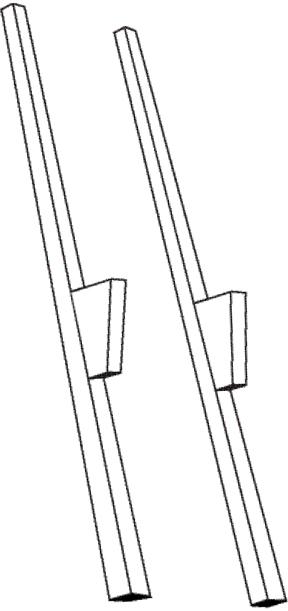
Aphasia is typically diagnosed using the Boston Diagnostic Aphasia Examination, a series of tests that assess basic language function. In one part of the exam, called the Boston Naming Test, patients are shown simple line drawings of common objects—such as a mask, a pair of stilts, a harmonica—and asked to name them. Responses are recorded, compared against an answer key, and the patients are scored. Simple, right?
According to Hall, the psychiatrist had examined the data and was troubled by an odd pattern: patients from the South tended to fare worse than those from the Midwest. But even responses from Midwesterners could be considered “wrong” if they were not deemed to be standard by the northeastern test-makers. Southern patients, for example, often said tommy walkers when shown a drawing of stilts, and would identify a harmonica as either a harp or a French harp. Midwesterners, on the other hand, often called the harmonica a mouth organ. After scouring old tests, the psychiatrist and his colleagues estimated that 13 percent of nearly 1,400 patients given the Boston Naming Test had been mis-scored, an outcome, says Hall, that may have subjected them unnecessarily to courses of language therapy. The physicians presented their findings at the International Neuropsychological Society in 2000.
Hall says she was pleased to note that the 2001 edition of the naming test’s answer key had added a few variants, including false face for mask, and harp and mouth organ for harmonica, as acceptable alternatives; she hopes that efforts to broaden the recognition of regional variation will continue.
“You simply can’t rely on an answer key that doesn’t allow for variation,” says Hall. “This drives home the fact that we can’t assume that our language is what everybody else speaks.”
Crossword Puzzles
The multicultural makeup of the United States brings with it a diversity of verbal expression that the increasingly professionalized field of medical interpretation is helping to decipher. For the past 14 years, Dharma Cortés, an HMS clinical instructor in sociology in the Department of Psychiatry at Cambridge Health Alliance, has been training people in medical interpretation.
After receiving a doctorate in sociology, Cortés spent two years studying medical anthropology in the HMS Department of Global Health and Social Medicine. Anthropology has served her well, because medical interpretation requires more than bilingualism. The interpreter must be a cultural broker as well as someone who can translate the languages being spoken in the clinic, including the argot of biomedicine and health insurance.
“Think of the situation from the patient’s perspective,” Cortés says. “You go to the doctor because you sense something is wrong. During the visit you might learn something new about yourself. Something about you or your life needs to change. That triggers anxiety. On top of this, there is a language barrier that requires the presence of a complete stranger who must interpret the deeply personal information you provide to the doctor. It can become very confusing. Any misunderstanding can adversely affect the patient’s follow-through when she goes home.”
Cortés has witnessed firsthand the fumbling of such communication. Once, she observed a community health worker—not a trained medical interpreter—tell a patient that her blurred vision was the result of diabetic retinopathy. The worker translated, “You have diabetes in your eyes.”
“So the most important thing,” says Cortés, “is to render a complete and accurate interpretation, not one that includes only what the interpreter thinks is important. You can’t distort, omit, embellish. For example, if the patient says, ‘I have a pain that comes and goes,’ the interpreter can’t abbreviate to ‘I have a pain.’ What seems like a small omission can have tremendous diagnostic implications.”
Descriptive Elements
Sonya Shin ’97, an HMS assistant professor of medicine at Brigham and Women’s Hospital, practices medicine in Gallup, New Mexico, a small city that borders the Navajo Nation. Her job is to train community health workers to work with members of that nation in all areas of health and preventive medicine. Shin herself is not a tribal member, nor is she fluent in Navajo, part of the Athabaskan family of languages. Navajo, in fact, has more speakers than any indigenous language of the United States or Canada. If language is more than a mere communication medium for symbols and sounds, the Navajo tongue is truly an entire cultural landscape all its own.
Shin has worked with Spanish-speaking patients in Boston, and she has worked in Russia as well. Her observations have led her to conclude that linguistic differences seem to track with cultural ones. The larger the divide between another language and your own, the greater the chance of all sorts of misunderstandings. Take, for example, the phrase “palliative care.” You might know the precise translation, but to the Navajo, simply bringing up the subject of death is taboo. And that leads to what is perhaps the deepest difference between Navajo and almost any other language in the West: words contain a sort of residential power. By speaking something, you might be summoning that very thing.
The first thing that Shin noticed when she began working with the Navajo was how their language was far more descriptive than English. The Navajo equivalent for “cancer” can roughly be translated back into English as “a cell that comes from a healthy cell but becomes unhealthy.” Much of the language is like this—indirect and descriptive of a process.
“If I’m talking with a patient,” says Shin, “and I tell him that if he doesn’t take his medication he might have complications with his kidneys, a Navajo person, at a cultural level, might take that to mean that I am essentially willing it to happen. Instead, I would have to tell him how other patients I’ve taken care of, people who share this same condition, have found that when they don’t take their medications, they have complications. You simply can’t speak about prognosis in a direct way.”
Nor can you look someone directly in the eye, a gesture taken as a challenge. For anyone raised in a Western society where frankness is a sign of virtuous courage, learning to become verbally and physically oblique might as well be learning another tongue.
“I have really grown to appreciate how some cultures place such power in the spoken word,” says Shin.
Spellbound
Shin may have had to travel across the country before experiencing cultural vertigo, but sometimes it comes to you.
In his early days as an intern at Duke, Kelling had gotten to know a young Haitian man who repeatedly showed up in the emergency department, each time with vague symptoms. He was nervous, anxious, depressed, losing weight. He couldn’t sleep, couldn’t eat. Kelling and his fellow physicians had no idea what was wrong.
Then, one night, the patient’s mother came in with him. She pulled Kelling aside and said, “He’s sick because a witch doctor put a hex on him. We need to get another witch doctor to take the hex off.”
Kelling told her he didn’t know of any local witch doctors, to which the mother replied, “I do,” and gave him a phone number.
Kelling shrugged, but with nothing to lose, he called the number and arranged for the alleged healer to visit the emergency room.
“That’s really the only time in my professional life that I’ve had to call a consultation with a witch doctor,” he says.
Soon the man arrived, a surprisingly unassuming person who, Kelling says, you wouldn’t consider twice if you passed him in public. The witch doctor spent a few moments alone with the young man in the examination room, and, when he emerged, he simply said, “It’s taken care of.” He left, and the young man was fine. The weight of the world had been lifted from him.
No one knew what had transpired, and to this day, it remains an unspoken secret. To the doctors, “it” remains untranslated.
David Cameron is the director of science communications in the HMS Office of Communications and External Relations.
Image: Mattias Paludi (top)