Who Will Care for Cancer Survivors?
A growing number of patients living with and after cancer are shuffled between oncology and primary care. Can survivorship be transformed for both patients and physicians?
- 12 min read
- Perspective
Illustration: Mark Weaver

Illustration: Mark Weaver
Kate is a software engineer, mom, and cancer survivor — though she might hesitate to define herself with that last term. After a hike one summer day her hip began to ache. Soon the pain was so searing it woke her from sleep. An X-ray showed it wasn’t bursitis, as her primary doctor initially suspected, but a rare bone tumor called osteosarcoma. She underwent a seven-hour surgery that removed a good portion of her femur and replaced it with a prosthetic. This was flanked by six cycles of grueling chemotherapy. She slept fourteen hours a day, vomited frequently, and was hospitalized several times to receive IV fluids.
Six months later, a chest CT to ensure she was in remission caught the tip of her adrenal glands. There looked to be a mass, the radiologist noted. Kate felt numb. She knew osteosarcoma could metastasize even after all the treatment she had received. She tried to remain calm as she methodically went through the next steps. Another CT scan focused on her adrenal glands, and there it was: a tumor the size of a grapefruit. Her surgeon conferred with her oncologist and decided to go straight to surgery, as a biopsy could spread cancer cells with the needle. When the pathology results came back, there was good news and bad news. The good: It wasn’t metastatic sarcoma. The bad: It was a new, second cancer, adrenal carcinoma.
It was then that her oncologist referred her for genetic testing. Kate had two rare cancers before her fortieth birthday. Did cancer run in the family? Kate didn’t know — she wasn’t close with her family. The genetic test came back positive for Li-Fraumeni syndrome, an inherited condition involving a mutation in a gene called TP53. Colloquially called the guardian of the genome, TP53 is responsible for repairing genetic errors that could lead to cancers. With that mechanism impaired, the lifetime risk of cancer is over 90 percent. Many, like Kate, are diagnosed young. Many develop more than one cancer.
I met Kate in Stanford’s Primary Care for Cancer Survivorship program, a clinic I codirect that provides comprehensive primary care for patients along the cancer continuum. My clinic is a landing pad for four groups: 1) survivors of childhood cancers who have reached adulthood, 2) survivors of adult cancers who have completed treatment, 3) adults receiving ongoing cancer-directed therapies, including those living with metastatic disease, and 4) “previvors” — people who haven’t been diagnosed with cancer but who carry an inherited genetic mutation, such as Li-Fraumeni, conferring elevated risk for developing it. In addition to the primary care practice, I see survivors and previvors in a consultative role, where I help bridge the gaps between their cancer care and primary care.
At our first visit, Kate came with many questions. Her hip still ached, her brain felt foggy, and chemotherapy had pushed her into an accelerated menopause. Were the drenching night sweats she was experiencing related to that or suggestive of something more sinister? Her abdomen felt numb over the surgical scar — would it stay that way forever? When should she test her children, now 8 and 6, for Li-Fraumeni syndrome?
As we got to know each other, more concerns bubbled to the surface. She took stock of all the radiation she received before she learned about her genetic risk and ruminated on what cancers might have been provoked. Her relationship with her husband was fraying, she feared, as the emotional energy flowed one way since cancer entered their lives. The medical bills hit right as she had to cut back at work.
And, there was the question underlying all the others: How should she live, knowing cancer could strike again at any moment?
Becoming a champion

I never envisioned a career where I could provide comprehensive, ongoing medical care to patients like Kate. In residency I was torn between primary care and oncology. Both encompass the medicine I value most: care for the whole patient, diagnostic complexity, a mix of emergencies and longer-term follow-up, and space for hard conversations. I pursued fellowship in hematology and oncology because I imagined becoming an oncologist was as close as I could get to being a primary doctor for patients with cancer.
But oncologists, I learned, are very much specialists whose expertise lies in treatment. When new problems landed in gray zones, I watched as oncologists advised patients to see their primary care physicians while primary care physicians told patients to ask their oncologists. I saw patients suppress concerns because of external and internalized pressures to celebrate cancer-free scans. I didn’t have the language of cancer survivorship at the time. What I saw were unmet needs.
I was independently discovering what the literature has been sounding the alarm on since 2006, when the Institute of Medicine (IOM) published the report From Cancer Patient to Cancer Survivor. The report recognized survivorship as a distinct phase of the cancer spectrum, acknowledged the need to improve education of providers about survivorship, and called for the dissemination of survivorship care plans to inform patients about what to expect after treatment.
Even earlier, in 1986, the advocacy organization National Coalition for Cancer Survivorship (NCCS) generated the language for survivorship we still use today. A cancer survivor, the NCCS said, is any individual who has experienced cancer from the day of diagnosis. Notably, family members, friends, and caregivers were also included in the definition.
Other papers delineated the gaps between oncology and primary care. “I have not found a provider who understands both sides of my current needs,” one survivor was quoted as saying in a 2010 study. “Internists do not understand my cancer and oncologists do not understand my noncancer health maintenance needs, such as monitoring cholesterol and blood pressure.”
But despite these clarion calls in the literature, I found that survivorship in practice was limited and ad hoc. I saw how living with or after cancer is given short shrift compared to treating cancer — both with health care dollars and cultural norms. “It takes a champion,” one physician who led a successful program advised me.
After completing my fellowship in 2021, I wanted to leverage my expertise in medical oncology, hematology, and internal medicine to be a one-stop shop for the cancer survivor and previvor. A few years earlier, a primary care physician and my now codirector, Jennifer Kim, under the guidance of Stanford’s Director of Cancer Survivorship, Lidia Schapira, piloted survivorship visits in the primary care setting. I joined the Stanford Primary Care faculty to establish my clinic with a slightly different practice model. I drew inspiration from geriatrics; just as a geriatrician is a primary care physician with a focus on older adults, I would be a primary care physician with a focus on patients with cancer. The only similar model I could find was the Primary Care for Cancer Survivors Program at Johns Hopkins. Its founder, Kimberly Peairs, kindly walked me through the lessons they had learned.
I quickly built a clinic of about three hundred cancer survivors and previvors within my approximately thousand-patient primary care practice. I treat more than one hundred others in my consultative role, where I continue to see new patients weekly. I see patients with all cancer types, from the most common breast and colon cancers to the rarest leukemias and sarcomas. I see entire families with hereditary cancer syndromes such as BRCA and Lynch syndrome. My work is both reactive — evaluating any new symptoms patients notice and interpreting them within the context of their cancer history — and proactive — reviewing that history and laying out plans to catch issues before they become problems. Survivorship means untangling what was caused by cancer or its treatment from what is not. It means improving what can be improved, while helping people navigate a new normal.
There is the 63-year-old writer who survived breast cancer. For two years she followed her oncologist’s advice to the letter and took a daily hormone blocker that kept her cancer in remission but also torpedoed her productivity and mood. She was advised to continue for five years total, but could she really take another three years of this? We reviewed her early stage, low-grade cancer and calculated her 10-year chances of survival to be 87 percent without the medication and 89 percent with it. With that data in hand, she felt empowered to stop. We monitor closely with mammograms and physical exams. Energy restored, she recently finished writing her fourth book.
There is the 50-year-old athlete who completed months of surgery, radiation, and chemotherapy for breast cancer. Monitoring her overall health meant keeping an eye on lung nodules noted incidentally on one of her many scans. One afternoon her CT scan revealed not only nodules but enlarged lymph nodes. I asked how she was feeling. “Not great,” she admitted. For the past few weeks, she had felt exhausted by her usual bike ride. Then she noticed gum bleeding. I immediately ordered lab tests. When two blood cell lines returned abnormally low, I called my patient and told her to go straight to the emergency department. The next day, the flow cytometry I ordered confirmed my fears: an aggressive leukemia called t-AML (therapy-related acute myeloid leukemia), precipitated by the very treatment that cured her breast cancer. Her life is radically changed after surviving her secondary cancer, but, miraculously, she is back to biking ten miles a day.
There is the 22-year-old lymphoma survivor who — haunted by a long ICU stay, countless lumbar punctures, and not knowing whether he’d live to see his high school graduation — stopped coming to medical appointments entirely. Just walking into a medical building like mine caused him tremendous anxiety. His sleep was wrecked. Once worried about being underweight, he was now fifty pounds overweight. I connected him with a support group, and he agreed to try antidepressants. With the energy to tackle other issues, we scheduled a litany of vaccines that he needed to redo after his bone marrow transplant. Now we’re working on weight; we figured out that radiation to the neck had caused hypothyroidism, making it difficult to drop pounds. We have reduced the number of specialists he sees from four to one, eliminating at least one obstacle that made recovery after cancer so daunting.
In each case, I imagine the alternative. What if our clinic did not exist? Perhaps the first patient would have accepted a major professional hit as par for the course for clean mammograms. The second may have been referred to a hematologist as an outpatient, resulting in dangerous delays that could have caused a life-threatening bleed. The third might have continued to suffer alone, in more ways than one. Of course, I can’t say any of this for sure. But I can imagine, because I’ve seen similar outcomes in those who lack survivorship care. And they are often missed by quality metrics in oncology that focus on remission and longevity, as well as those in primary care that use a one-size-fits-all approach to things like vaccines and cancer screenings.
Studying the model
After about a year in practice, I knew the only way to improve the new model of primary care and survivorship wrapped into one clinic was to put it under a microscope. I assembled a team to help me study the clinic’s successes and shortcomings. Where were we helping, and what continued to be missed?
Step one was creating a database. My colleague Natasha Steele and I formulated a list of common survivorship issues: cancer-related fatigue, neuropathy, cognitive changes, bone health, fertility, sexual health, cardiovascular risk, goals-of-care discussions, genetic testing, immunizations, surveillance for the original cancer, screening for secondary cancers, lifestyle counseling, and mental health. Then we scoured charts to see if those needs were being met. We published data showing the feasibility of the combined primary care–survivorship model. Long-term effects — defined as those that began during cancer treatment and persisted — and late effects — defined as those that cropped up later — were addressed in 87 percent of patients, while at least one other primary care issue was managed in 96 percent.
Next we parsed data by group. My colleague Maya Ramachandran led an analysis of geriatric patients. We learned that 28 percent of patients in the clinic are over age 65; among those, 40 percent have active cancer. They average 2.8 visits per year split between in person (61 percent) and video (29 percent) or phone (10 percent), representing multiple avenues to engage a patient population requiring more touch points.
A senior resident, Ellen Zhang, MD ’23, compared survivorship needs addressed among patients with blood cancers to those with solid tumors. We learned that cardiovascular risk, fertility, and cancer-related fatigue were addressed significantly more often, while sexual health was managed less often.
Why that is remains to be determined. But just seeing these results led to a partial fix. For example, I updated my note template to broach sexual health in blood cancer survivors, and I make sure we offer phone calls and video visits to older patients. We are currently working on an analysis of adolescents and young adults compared to adult survivors. We are also in the midst of a quality improvement project studying how survivors in the clinic navigate their care. We designed a questionnaire that asks: Do patients feel empowered to manage long-term symptoms? Do they know when to seek care for new ones? Do they know who to call?
From champions to programs
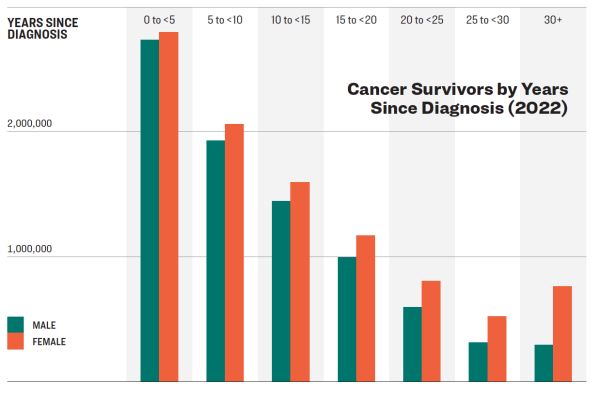
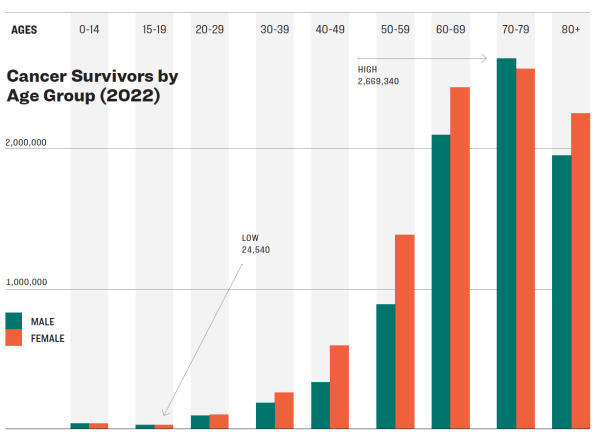
To me, these health systems gaps remain the most motivating ones. Patients must know who to call, and, on the other end, we need a workforce to pick up the receiver. The National Cancer Institute projects that there will be 26 million cancer survivors by 2040. Many of these will be young people, who are getting diagnosed at higher rates now compared to previous generations.
Recently, I was interviewing medical students applying to residency at Stanford. Over and over again I spoke to applicants interested in cancer survivorship as a career. I was happily stunned. These students were speaking a language I had barely heard until my fellowship. That there’s this much interest so early in the pipeline means something in our public messaging is working. Yet I tell them the truth: There is still no career path. I invite them to join me in my clinic, where I frequently host residents. I echo the line I was told: that it takes a champion. Then I ponder — how can we transform cancer survivorship from an ad hoc network of champions into a formal branch of medicine with training, standards, and access?
I have some ideas: a one-year, nationally accredited cancer survivorship fellowship that teaches the subject directly, rather than as a Post-it note tacked onto an oncology fellowship. Elective rotations for junior and senior residents. And, at the bare minimum, a billing code — as of 2025, there remain no survivorship-specific codes to ensure these visits get covered. Then there are more ambitious goals, including team-based survivorship clinics — a model we know works in medicine more broadly — with important players such as a nutritionist, social worker, and physical therapist working together to help survivors.
We must also find creative ways to support general practitioners who see cancer survivors every day. Last year my codirector Jennifer Kim and I teamed up with Regina Jacob from Northwell Health and gave a workshop on survivorship pearls at the Society of General Internal Medicine Annual Meeting, one of the largest national conferences for internists. I regularly teach high-yield survivorship concepts at Stanford along the training spectrum from medical students through residents and fellows to attendings. This year we are piloting “e-consults,” where we will guide providers through chart review and remote care.
I recognize the obstacles. Working within the U.S. health care system means navigating a wider ecosystem of fragmented care; we wrestle with barriers such as unshared medical records, payment models that reward short visits, and hyperspecialization (something I wrote much more about in my 2023 book Fragmented: A Doctor’s Quest to Piece Together American Health Care). Primary care desperately needs to delegate bureaucratic tasks so that the important work of caring for survivors does not feel like another chore that busy doctors have no time to do. But even as we advocate for broad systemic change, there is much we can do now to embed a survivorship lens into routine medical care.
Take Kate. While fear of cancer’s return may prevent her from ever fully identifying as a survivor, she has found a way to live. She learned to walk the tightrope of staying aware of new symptoms while not letting thoughts of cancer consume her. She let herself plan ahead — first in months, then in years. Together, we speak candidly about living in uncertainty. We interpret unexpected findings on MRIs. We triage new problems within the context of her medical story.
The last we met, that new problem was headaches. Three days earlier she stood too quickly and struck her head against an open freezer. She had the welt to prove it, and the pain was throbbing and persistent. I did a focused neurologic exam. I recommended Tylenol and ice packs, and she recovered well at home. I quietly picture what might have happened if our clinic didn’t exist. I could see an urgent care or primary care doctor sending Kate straight to the emergency department for a head CT — something relatively benign for most but dangerous for someone with Li-Fraumeni syndrome.
But then I imagine more hopeful alternatives. What if a survivorship e-consult offered time-sensitive advice to a primary care doctor? What if an experienced nurse practitioner on a survivorship team evaluated Kate and carefully weighed a CT scan’s risks and benefits? The world of cancer survivorship is facing a unique moment with a combination of rising demand and supply; we must match them. The what-ifs no longer just trouble me about the worst-case scenarios. They give me hope for the best.
Ilana Yurkiewicz, MD ’15, is a clinical assistant professor at Stanford University School of Medicine, codirector of Stanford’s Primary Care for Cancer Survivorship program, and author of the book Fragmented: A Doctor’s Quest to Piece Together American Health Care (W.W. Norton, 2023). She graduated cum laude from HMS in 2015. Disclosures: Names and certain identifying details were altered to protect patient confidentiality. The author is a strategic advisor to Previvor Edge and a consultant to OncoveryCare.
Research at Harvard Medical School hangs in the balance due to the government’s decision to terminate large numbers of federally funded grants and contracts across Harvard University.