The Covert Consciousness Dilemma
The discovery of hidden awareness in seemingly unresponsive patients is raising pressing questions in brain injury care
- 11 minute read
- Feature
Illustration: Valerie Chiang

Illustration: Valerie Chiang
Brian Edlow has cared for countless patients in a coma. But there’s one phenomenon that still gives him the chills every time he experiences it: the moment a previously unresponsive patient shows the first hints of consciousness.
Edlow, now a critical care neurologist and an HMS associate professor of neurology at Massachusetts General Hospital, remembers the first time it happened. He was a medical student, and his patient, a young man, was unconscious after being hit by a car while riding a bike. The man had been unresponsive for two weeks. But that morning, Edlow grasped the patient’s hand and asked him to squeeze it — and the young man squeezed back.
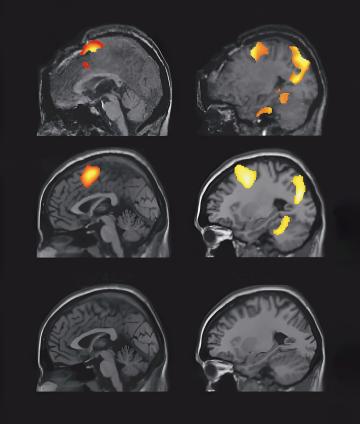
Around the same time, Edlow heard about a paper published in Science that stunned him. The 2006 study focused on a patient who sustained extensive brain injuries following a traffic accident. Six months later she was still in a vegetative state. She showed no evidence of purposeful behaviors, such as following commands or making intentional movements. But then the researchers put her in an fMRI machine. While scanning her brain, they asked her to imagine walking through her house, moving slowly from room to room. And they told her to imagine playing a game of tennis, swinging for the ball with forehand and backhand strokes.
Photo: Heather McGrath
What the researchers saw on the scan was a bit like Edlow’s hand squeeze, but rendered in colorful 3D pixels. Her brain responded to the commands with activity patterns that matched those of a healthy person, as if to say, I’m still here.
“This just blew my mind,” recalls Edlow. “It completely reframed the way that we think about consciousness and opened up the possibility that a substantial number of patients may be conscious even if we cannot detect purposeful behavior at the bedside.”
He didn’t know it then, but nearly two decades following those formative experiences, his research would help to reveal that at least one-quarter of seemingly unresponsive patients with brain injury harbor evidence of awareness on brain scans. Today, he and colleagues at HMS and beyond are working to improve methods of detecting that phenomenon, known as covert consciousness, and to untangle the thorny scientific, ethical, and clinical questions that it poses.
Charting Consciousness
When treating patients with brain injury, Edlow and other doctors have always faced a conundrum: To infer how conscious a person may or may not be, they rely on what they can observe from the outside.
They use bedside exams to walk patients through tasks, looking for hints of arousal or awareness. Then they determine, based on standardized scales, which “disorder of consciousness” a patient has. “I’ll sort of go up the ladder,” explains Joseph Giacino, an HMS professor of physical medicine and rehabilitation at Spaulding Rehabilitation Hospital, who developed the Coma Recovery Scale–Revised, one of the most widely used scales, in the early 2000s.
First, he’ll check if the patient purposefully responds to any stimulus, like turning in the direction of his voice. If they remain totally unresponsive and their eyes stay closed, they’re in a coma. Within about two weeks of injury, most patients open their eyes, but if they still don’t respond to stimuli on purpose, they’re considered to be in a vegetative state. If they start showing signs of awareness — brushing hair from their eyes, squeezing a hand when prompted — they’re in a minimally conscious state.
When is a patient considered conscious? There are two “exit criteria,” Giacino explains: They can give reliable and consistent responses to a series of six consecutive yes or no questions, and they can use an object functionally — for example, putting a cup to their mouth.
These diagnostic labels are important. Outcome predictions, rehab plans, and even life-and-death choices depend on them. But exams that rely on observable behavior can’t always capture a patient’s subjective experience. That fact came into sharper focus once researchers began employing advanced imaging technologies to glimpse inside the brains of unresponsive patients.
The question is, once you identify someone as being covertly conscious, what now?
The first such studies, in the late 2000s, used fMRI, which maps the flow of blood to active brain regions, translating those shifts in thought into bursts of color. Then researchers started experimenting with electroencephalography, or EEG, which records the rhythmic firing of neurons through small electrodes placed on the scalp. Both tools are now used to detect covert consciousness because they let researchers see the neural signature of a thought, even if the body remains still.
“What’s really interesting about the brain is that when it’s imagining doing something, it acts in the same way as it does when it’s actually doing it,” says Giacino. “For both EEG and fMRI, the patterns of electrical activity, or the blood flow changes, have a sort of signature that says, ‘This person’s doing or imagining doing the task.’ We know that because we’ve done the task with people who are perfectly healthy.”
A Silent Minority
The tasks used in the 2006 study — imagining a tennis match and visualizing the rooms of one’s home — were not chosen at random; these prompts are known to reliably activate distinct patterns in healthy brains. And when researchers looked at that one patient’s fMRI scans, the images were indistinguishable from those of the healthy controls.
“That really stunned me. I think it stunned a lot of people,” says Yelena Bodien, an HMS lecturer on physical medicine and rehabilitation, part-time, at Spaulding, and an assistant professor at Vanderbilt University Medical Center. She decided to pivot from studying schizophrenia to disorders of consciousness when she first learned about the research.
That first paper focused on just one patient. In the following years, as researchers recruited more participants, they identified additional patients with signs of covert consciousness. But those studies were still relatively small and in siloed research groups. A few years ago, Bodien helped organize a group of 30 international researchers, including Edlow and Giacino, to publish what she calls “a kind of magnum opus in a large sample.” The researchers sought a more reliable estimate of how many patients might exhibit “cognitive motor dissociation,” a type of covert cognition specific to patients in coma, vegetative state, or minimally conscious state who do not follow bedside prompts, like squeezing a hand or giving a thumbs-up, but do follow prompts that are detected on brain scans.
Their study, published in the New England Journal of Medicine in 2024, found that among 241 adults who could not follow bedside commands, 60 (about 25 percent) could follow cognitive tasks in the fMRI scanner or during EEG testing, suggesting that they could think and understand despite being unable to demonstrate it with their bodies. These patients spanned different injury types — from traumatic brain injuries to stroke to cardiac arrest — as well as recovery stages, from acute to chronic. “There was not a subset of patients in which we didn’t find this phenomenon at all,” Bodien says.
The study also included 112 patients who could follow commands at the bedside. The findings among these patients are what surprised Bodien most: 69 of those clearly conscious patients (over 60 percent) did not generate the necessary signals on fMRI or EEG to pass the brain scan tests. In other words, even patients who show outward signs of consciousness can struggle to pass the tests. That suggests the tests are demanding enough to miss some conscious people — and that cognitive motor dissociation could be even more common than the reported 25 percent.
While the tests don’t necessarily show the upper limits of a patient’s cognitive capacity, the researchers say that demonstrating those responses to commands on brain scans requires a meaningful level of awareness. “There’s probably a broad spectrum of levels of consciousness that individuals with this diagnosis have, but many of us feel confident that if somebody can do these tasks, their level of consciousness might be quite high,” Edlow says. “The question is, once you identify someone as being covertly conscious, what now?”
High Stakes, Low Clarity
In the ICU, where Edlow spends his time, even just the awareness that an unresponsive patient could be conscious has immediate implications. Research suggests that 70 percent of ICU deaths from traumatic brain injury result from the withdrawal of life-sustaining therapy, often within the first three days. “A substantial proportion of people die in the ICU because it’s assumed that they have minimal or no cognition and that they’re not going to recover,” Bodien says. “The ventilators are turned off and the patients die.”
Even patients who are kept alive but remain unresponsive tend not to meet relatively stringent criteria for admission to rehabilitation facilities. As a result, they usually end up in long-term care settings with limited access to helpful interventions.
If consciousness can’t be ruled out, the calculus changes. Michael Young, MD ’16, an HMS assistant professor of neurology at Mass General, says that a patient’s level of consciousness weighs heavily in the decisions families and clinicians make about whether to continue life-sustaining care and what kinds of treatments to pursue. “That really speaks to the centrality of consciousness to our concept of personhood and, for many, what makes life worth living,” he says.

Photo: Heather McGrath
The most obvious question decision-makers ask is whether exhibiting covert consciousness means that someone is more likely to recover. The evidence so far is mixed. Some studies have found that its presence does not predict prognosis. But research in acute settings shows more promising links. A 2019 study by researchers at Columbia University found that among patients in the ICU, 41 percent of those who showed signs of cognitive motor dissociation shortly after injury reached functional independence within a year — for example, they were able to eat, go to the bathroom, and get dressed — compared with only 10 percent of those who did not.
Yet outside of a few specialized centers like Mass General, most patients worldwide still lack access to the technologies required to undergo these tests, as well as to the experts needed to interpret them. Mass General’s Emerging Consciousness Program, co-led by Edlow and Young, is tackling both of these limitations at once. In addition to offering extensive fMRI and EEG evaluations, they’re enrolling patients in clinical trials designed to ensure the science is strong enough to guide care. They’re confronting the field’s most pressing questions, such as how to standardize testing, how to reconcile results when fMRI and EEG contradict one another, how to optimize testing characteristics, how to talk about results with families, and what treatments should follow when covert consciousness is detected.
To expand access, the program currently offers “TeleConsciousness” assessments to provide expert guidance and second opinions remotely. Ultimately, Edlow and Young envision a “hub-and-spoke” model in which data could be acquired at community hospitals nationwide and then interpreted by Mass General experts.
Unlocking Voices
For now, though, even those who have access to tests still face fraught decisions. “I think it’s not all that helpful to physicians or to families to say that their loved one is conscious and that’s it,” says David Fischer, MD ’16, an assistant professor of neurology at the Hospital of the University of Pennsylvania. “The logical next question after you infer that someone is conscious is to say, ‘Well, how do we actually communicate with them?’ And we haven’t been able to answer that question.”
But researchers are trying. Some have attempted using the typical visualization tasks to ask patients questions — for example, by asking them to imagine playing tennis for “yes” and navigating rooms for “no” — but that approach has only worked on rare occasions.
Fischer has been testing a novel technique that could both improve detection of covert consciousness and facilitate communication with those who experience it. Called neural decoding, the method exposes a patient to different stimuli — sounds, words, images — while scanning their brains using fMRI or EEG. Researchers use machine learning to analyze brain patterns that consistently happen when that individual sees or hears a certain thing. Then, when exposed to new stimuli, the algorithm “reads” the person’s brain activity to decode what they’re experiencing. The hope is that someday a computer might translate those thoughts into text or sound.
The reality is that the evaluation of consciousness is an inherently gray and somewhat abstract thing.
Another promising technology is the brain-computer interface. Researchers have had some success enabling communication in patients with “locked-in syndrome” — cognitively normal but paralyzed by conditions like ALS or stroke — by putting microelectrodes on the surface of the brain to turn thoughts into action. Eventually, Edlow says, this technology might progress enough to facilitate communication with patients with disorders of consciousness.
By understanding what causes a state of covert consciousness, scientists might also be able to find treatments that help patients recover. Some evidence suggests that the phenomenon involves damage to the thalamocortical motor fibers, which act as a bridge between the thalamus, the brain’s central relay station, and the cortex, which handles high-level thinking and movement planning. Young just enrolled the first participant in a new study that will test the use of focused ultrasound to stimulate the thalamus and restore its communication with the cortex in a noninvasive way. To gauge the effect, he’ll use the same fMRI and EEG mental imagery tasks that detect covert consciousness — this time as biomarkers of response and not just diagnostic tools.
No Evidence of Absence
In addition to exploring treatment strategies, Young spends a lot of time untangling the ethical questions that covert consciousness raises: Is there a moral duty to test for it? Does sharing uncertain findings create false hope? How can clinical trials enroll patients who may be conscious but unable to provide traditional consent?
Young earned a master’s degree in philosophy before attending medical school, so he’d already spent years pondering big questions about consciousness and personhood. He recalls being struck by how medicine tended to neatly “define and operationalize” concepts of consciousness that philosophers and ethicists had grappled with for ages.
Perhaps not coincidentally, Fischer also has a background in philosophy. It helps him feel more comfortable facing concepts that defy easy explanation. “I think physicians by nature like things to be in neat buckets,” he says. “But the reality is that the evaluation of consciousness is an inherently gray and somewhat abstract thing.”
The more he’s learned about covert consciousness, the humbler Fischer has become about making assumptions. Families of patients often ask him, “Do they know I’m here?” He tells them he doesn’t know, because current tests can rule in the presence of some level of consciousness, but they can’t completely rule it out. The most important lesson to glean from this research, says Fischer, is that it is often impossible to know for sure that a person is unconscious.
Young has recently been interviewing patients who have recovered from states of covert consciousness, trying to learn about their point of view. He spoke with one man who vividly recalled experiences and conversations he’d heard at times when others did not realize that he was cognizant. Perhaps if that man’s consciousness had been detected, he would have been treated differently at the time, sparing him “memories that remain traumatic to him to this day,” Young says. “That case, even if an outlier, underscores the importance of diagnostic humility.”
Humility is an understandable response to a phenomenon that currently raises more questions than answers. But with the science advancing, what these researchers discover about covert consciousness could ultimately transform how patients with brain injury are understood, cared for, and treated.
“These advances are coming at a really exciting time,” Young says. “There is a clinical and ethical imperative to unlock the voices of people who are there but cannot speak for themselves.”
Molly McDonough is the associate editor of Harvard Medicine.