Functional Neurological Disorder, Reframed
Science sheds new light on a disorder that medicine forgot
- 11 minute read
- Feature
Illustration: Valerie Chiang

Illustration: Valerie Chiang
Mark Hallett, whose work is described here, passed away as the story was being prepared for publication. A tribute to his life and work is available on the website of the Functional Neurological Disorder Society, the organization he cofounded to improve the understanding and treatment of FND.
Like any neurologist, Mark Hallett, MD ’69, often encountered symptoms he couldn’t easily explain.
A patient might show up in his clinic with one-sided limb weakness that came and went, or a hand tremor that varied in frequency and speed. Another would develop an unusual gait or be suddenly unable to walk. Still others experienced slurred speech patterns and involuntary movements. Then there were the convulsive episodes: scary events involving full-body shaking that resembled seizures. These symptoms could be debilitating and endure for years. But routine tests like MRI or EEG appeared normal.
By the early 2000s, Hallett calculated that around a third of the patients presenting in his movement disorders clinic at the National Institutes of Health were experiencing such unexplained symptoms. “I said, ‘Gee, that seems to be a pretty important consideration,’” he recalls. “But no one was really taking an interest in these patients. They never really got an idea of what their diagnosis was, and there was no research going on.”
The patients were suffering from what’s now known as functional neurological disorder, or FND, a condition that manifests in a range of neurological symptoms, from limb weakness to tremors to trouble walking and speaking. Its symptoms can resemble those of other neurological diseases such as epilepsy and Parkinson’s but can’t be explained by structural abnormalities on brain scans or other routine medical tests.
FND is not rare. So-called functional symptoms are among the most common reasons for patients to visit a neurology clinic, while research suggests that anywhere from a quarter million to five million people live with FND in the United States. It’s also not benign. Studies have found that patients with FND report levels of physical disability and mental distress comparable to those reported by patients with Parkinson’s and multiple sclerosis. One paper found that only around a fifth of patients achieve remission after seven years of treatment. Another calculated that people with functional seizures have a mortality rate 2.5 times higher than that of the general population.
Falling somewhere between neurology and psychiatry, FND has long occupied a gray area in medicine, its patients marginalized and misdiagnosed. Today that is starting to change as doctors like Hallett — as well as HMS researchers in specialized clinics at Massachusetts General Hospital and Brigham and Women’s Hospital — work to bring the condition out of the shadows.
Their research is revealing quantifiable brain changes in patients with FND. And it’s illuminating new insights into the brain, from how we sense what’s happening in our bodies and feel agency over our movements, to the role of attention, to how emotions are constructed — and how individual life experiences shape all of this.
“These are all cutting-edge, deeply meaningful issues,” says David Perez, MMSc ’16, an HMS associate professor of neurology and psychiatry and the founding director of the Functional Neurological Disorder Unit at Mass General. “They are intrinsically interesting and fundamental neuroscience themes. And they all sit in this one patient population.”
Symptoms and stigma
FND wasn’t an official diagnosis until 2013, when it appeared in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5). But “this disorder has been described for centuries,” says Barbara Dworetzky, an HMS professor of neurology and the A.J. Trustey Endowed Chair in Neurology at Brigham and Women’s.
In the late 1800s, famous French neurologist Jean-Martin Charcot chronicled FND-like symptoms among women institutionalized at Salpêtrière Hospital in Paris. But back then the preferred diagnosis was “hysteria.” That loaded label — originating in hystera, the Greek word for womb — grew out of an ancient belief in a “wandering uterus” and endured for centuries as a catchall diagnosis for symptoms in women that doctors couldn’t explain.
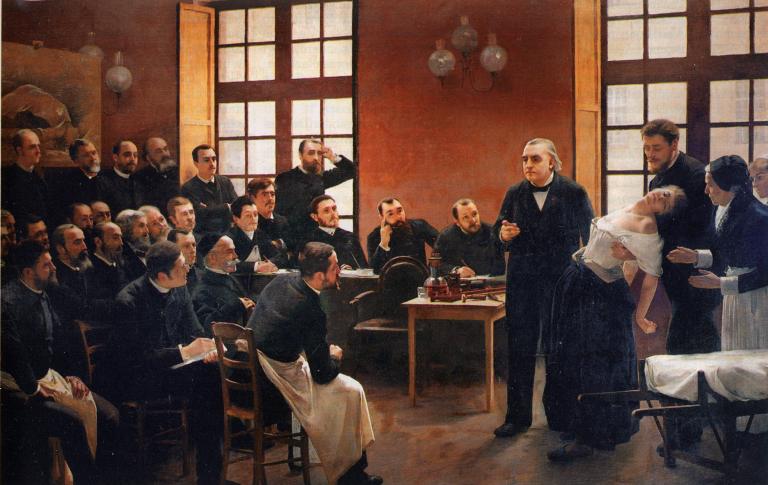
Charcot did suspect that many of his patients’ symptoms had neurological rather than uterine origins. But he couldn’t find any evidence of brain abnormalities with the tools available at the time.
Over the course of the 20th century, “the condition fell off the map because it was neglected,” says Dworetzky, an expert on functional seizures who co-leads the Functional Neurological Disorder Program at Brigham and Women’s. In part, that’s due to the legacy of the wandering womb. FND symptoms are more likely to afflict young women, whose medical concerns have so often been dismissed — although they can appear in men, too. In any case, Dworetzky adds, researchers really lost interest as new imaging technologies emerged, revealing no evidence of a mysterious brain lesion Charcot had hypothesized was involved. “People didn’t see anything on scans,” she says. “And seeing is believing, I guess.”
Instead, a different theory of the condition came to dominate, one first advanced by Sigmund Freud. A student of Charcot, Freud argued that hysteria was a psychiatric issue “converted” into somatic symptoms. That idea spawned the terms “psychogenic symptom disorder” and “conversion disorder,” which persisted until recently.
Doctors really did want to do the right thing, but this problem was complex and misunderstood.
The result of this thinking was that most neurologists tended to refer patients with these symptoms to psychiatrists. They were correct to suspect psychiatry could help; FND frequently overlaps with conditions like depression and post-traumatic stress disorder, and studies indicate that people with FND could have three to four times higher odds of identifying a prior psychological stressor or childhood adversity as compared to healthy controls. But these factors alone can’t explain the condition. Fewer than half of FND patients can identify a psychological trigger, and most people with psychiatric issues do not develop the neurological symptoms seen in FND.
So the patients would move on, but they wouldn’t get better. “They were lost in the system,” says Dworetzky. “Psychiatrists didn’t want to see them; neurologists didn’t want to see them.” Some charted their own course, collecting medications and diagnoses. Others lost trust in conventional medicine. “I think doctors really did want to do the right thing, but this problem was complex and misunderstood,” Dworetzky adds. “It wasn’t being taught and it wasn’t in curricula.”
The situation started changing when some doctors acknowledged their blind spots and began taking cues from patients. “The people with lived experience are really helping us,” says Dworetzky, “because they’re the ones with the disorder. For so long, we got it wrong.”
Agency, interrupted
Hallett was one of those doctors. He knew that researchers had not found evidence of quantifiable interruptions, such as lesions, in the brain and spinal cord pathways that control voluntary muscle movement in these patients. But he believed his patients when they told him they didn’t feel in control of what was happening to their bodies. If the movements were not “involuntary” in the traditional sense of a motor pathway interruption, he wondered, could something be hampering the patients’ sense of control?
Until scientists started studying people with FND, Hallett says, there hadn’t been much research into agency, the brain’s sense that “I did that.” Agency relies on complex feedback loops. Say you want to move your hand. Your brain needs to send a command not only to the muscles but also to sensory brain regions that predict what the results of the movement will be. When your hand moves, your brain receives signals based on what you sensed — “I saw it move,” “I felt it move” — to confirm it happened. If what you expected matches what you sensed, you get the feeling that you controlled the movement.

Photo: Courtesy of the European Academy of Neurology
Hallett began recruiting patients with functional tremors. “Their arm would go like this,” he says, hand trembling as he demonstrates the symptom. The patients described their tremors, which could come and go, as involuntary. But they could also intentionally mimic the movements on cue.
Hallett put the patients in an MRI machine and asked them to imitate their tremors. But as their brains were being scanned, they sometimes also experienced the involuntary tremors. Hallett was struck by what he saw: Different brain patterns occurred depending on whether patients intentionally produced the symptoms. Those differences pointed to the right temporoparietal junction, which showed altered activity and crosstalk with regions involved in motor control. It’s a part of the brain network involved in integrating predictions with sensory feedback — which helps us distinguish “I moved my hand” from “my hand moved.”
“When we reported that paper in 2010, investigators were very excited,” Hallett recalls. “It was the first evidence we had that shows that there are brain abnormalities in these patients, that it isn’t all just something that they make up.”
Hallett, who went on to found the Functional Neurological Disorder Society in 2018, devoted the later stages of his NIH career to researching and advocating for patients with FND. His work encouraged the rebranding of “conversion disorder” into “functional neurological disorder.” The new name reflects what scientists have started to understand: While the structure of the brain appears generally intact, the way it functions may be disrupted. It’s less of a hardware problem and more of a software glitch.
Brain patterns hint at FND causes
Perez says it’s difficult to overstate how instrumental Hallett’s work was in bringing FND out of the fringes. “To have somebody of his stature and rigor and international regard identify FND among the most interesting problems that he could roll up his sleeves and tackle was tremendous,” he says.
The intersections between neurology and psychiatry have always fascinated Perez. At the time of his training — which included residencies in both specialties at HMS-affiliated hospitals — so-called conversion disorder was a diagnosis of exclusion. Neurologists would say they’d found no evidence of stroke, epilepsy, or multiple sclerosis; psychiatrists would rule out acute suicidality, PTSD, or major depression. Perez wondered, what do these patients have?
Photo: Matt Kalinowski
He’s now spent more than a decade trying to answer that question. His team uses advanced techniques like resting-state fMRI and diffusion tensor imaging, which follows the movement of water in the brain to see how different brain regions communicate. In addition to patients with FND and healthy controls, their studies include psychiatric controls with mood or anxiety disorders to tease apart what FND shares with mental health conditions and what’s distinct.
The hints they’ve uncovered point to parts of the brain like the insula, the amygdala, and the cingulate gyrus. These are parts of the salience network: regions that help us detect what’s important inside our bodies and around us. FND patients, they’ve observed, tend to have increased crosstalk between these regions and areas involved in motor control. Perez’s team has also found that this relationship is dose dependent: The more severe the symptoms, the greater the abnormal connectivity.
They’ve also found that people with FND tend to have subtle structural differences, like small alterations in volume or thickness of particular regions, in parts of that network. In other words, FND may involve some tiny hardware alterations, too. These microstructural changes are significant enough that a machine-learning model Perez’s team developed last year successfully distinguished brain MRI scans of people with functional motor symptoms from healthy controls with 80 percent specificity.
Perez speculates that the differences he’s observed point to “increased noise in the system” and a hijacking of normal abilities that impairs movements that otherwise would be relatively automatic. The brain regions involved may vary somewhat from patient to patient. “If we have a software-crashing problem, there are many ways to scramble the system to get a crash,” he says.
Training in both neurology and psychiatry gives Perez a helpful vantage point to untangle why this might happen. He suspects that psychological triggers like traumatic events or physical triggers like concussions can thwart the brain’s ability to control and sense the body. When it’s predicting what we are about to feel, do, or sense, the brain draws from our past experiences. If those predictions are thrown off by emotional stress, a previous injury, or other factors, the brain can misinterpret normal signals, leading a person to experience movement they don’t feel in control of.
Each patient has to be treated with a “biopsychosocial” approach, Perez says, to untangle their unique triggers and risk factors. “When we think about software crashing or brain-mind-body overload, we want to individualize that,” he says. “Why might you be more at risk for glitches in connectivity patterns in your brain, or instances of brain-mind-body overload that result in physical symptoms?”
Treatments gaining traction
Describing this to patients isn’t always easy. But it’s an important first step in treating them. “The brain’s primary role is to keep us safe,” Dworetzky explains to her patients with functional seizures. In FND, the brain is “in an overwhelmed state, and the nervous system is getting too many inputs.” To return to a baseline of safety, she tells them, the brain invokes reflexive adjustments, such as a fight-or-flight response that can manifest as a seizure-like event. She’s careful to add that scientists don’t fully understand why this happens, but they’re learning more.

Photo: Matt Kalinowski
Dworetzky, who is now president of the Functional Neurological Disorder Society, also knows that many of her patients have been dismissed or misunderstood. “I make sure that I say, this is not your fault. You are not faking it,” she says. “I clearly say those things because they may have heard it implied in the emergency department or somewhere else. That implicit language can be really harmful — it not only gets patients away from care but it can also make them worse.”
It helps that FND is no longer a diagnosis of exclusion; today it’s based on positive signs. For example, if a patient has a tremor, a neurologist might ask them to move a different body part, like tap their fingers. If the tremor disappears or changes in rhythm when the patient directs their attention away, that suggests the movement is linked to the voluntary motor system rather than to structural nervous system damage. Or, a patient with one-sided leg weakness might not be able to push down their leg when prompted — but if asked to lift the opposite leg, the weak leg will push downwards quite well, revealing it does have strength. These features are not only helpful clues for doctors. They also serve as evidence for patients that recovery can be possible.
It’s fallen through the cracks because it’s at the borderlands. There’s this enormous clinical and research gap between neurology and psychiatry.
The most effective approaches to recovery, says Dworetzky, combine cognitive behavioral therapy with physical, occupational, and/or speech rehabilitation to identify personal triggers, teach coping strategies, and retrain the brain’s responses. It’s also important to treat any other comorbidities, like migraines or PTSD, that may trigger or worsen FND symptoms. The approach needs to be multidisciplinary. At both Mass General and Brigham and Women’s, for example, the FND clinics include neurologists, mental health professionals, psychiatrists, rehab doctors, physical and occupational therapists, speech therapists, and social workers. With a solid diagnosis and individually tailored treatment plans, many patients who would have otherwise fallen through the cracks are seeing improvements.
Perez says that in his clinic, he sees patients get better on a regular basis. “But we also need to be humbled that there are patients who are having suboptimal responses to the latest evidence-based treatments,” he adds. “There’s much more work to be done.”
The great disconnect
Indeed, recent studies suggest it still takes an average of two years for most FND patients to get a diagnosis. Those delays, misdiagnoses, and ineffective treatments strain health care resources. One study found that annual costs per U.S. patient in medical bills and lost productivity could reach $86,000, while another calculated that FND creates a $2 billion per year burden on the U.S. health care system.
Perez points out that for other complex brain disorders, there is a closer match between health care expenditures and the amount of government research funding invested. In contrast, funding for FND is minimal. “It’s fallen through the cracks because it’s at the borderlands,” he says. “There’s this enormous clinical and research gap between neurology and psychiatry that we still need to work on closing. Who should receive the grant? Is this a grant for mental health or neurology?”
That divide wasn’t always so huge. Back at Salpêtrière, Perez says, neurologists and psychiatrists worked side-by-side and learned from one another. Charcot had described “the neurological tree” with psychiatric problems and neurological diseases as different branches. The disciplines diverged over time, but FND can’t be understood using the framework of just one or the other.
“This is exactly the kind of condition that teaches us that the brain doesn’t separate into neurologic circuits and psychiatric circuits,” Perez says. “It challenges the artificial dualism between psychiatry and neurology and between physical health and mental health as robustly and directly as any condition.”
Molly McDonough is the associate editor of Harvard Medicine.